Breast cancer is now the most commonly diagnosed cancer among Indian women. Within that broad diagnosis, hormone receptor-positive, HER2-negative (HR+/HER2-) breast cancer accounts for approximately 60-70% of all cases — and for this large and clinically important group, the treatment landscape has been fundamentally transformed over the past decade by a class of medicines called CDK4/6 inhibitors.
Three CDK4/6 inhibitors are now approved, clinically established, and available in India — Palbociclib (Palbace), Ribociclib (Kryxana), and Abemaciclib (Ramiven). Each has a substantial Phase 3 evidence base, each is used in combination with endocrine therapy, and each has demonstrated clinically meaningful improvements in progression-free survival. But they are not interchangeable. Subtle and not-so-subtle differences in efficacy data, safety profiles, dosing, and approved indications mean the choice between them has clinical significance — particularly in 2026, when all three are fully integrated into Indian oncology practice and the question is not whether to use a CDK4/6 inhibitor but which one and when.
This article is a practical guide for Indian oncologists and patients navigating that choice.
What CDK4/6 Inhibitors Actually Do
Before comparing the three agents, it helps to understand why this class of medicines works so well in HR+/HER2- breast cancer.
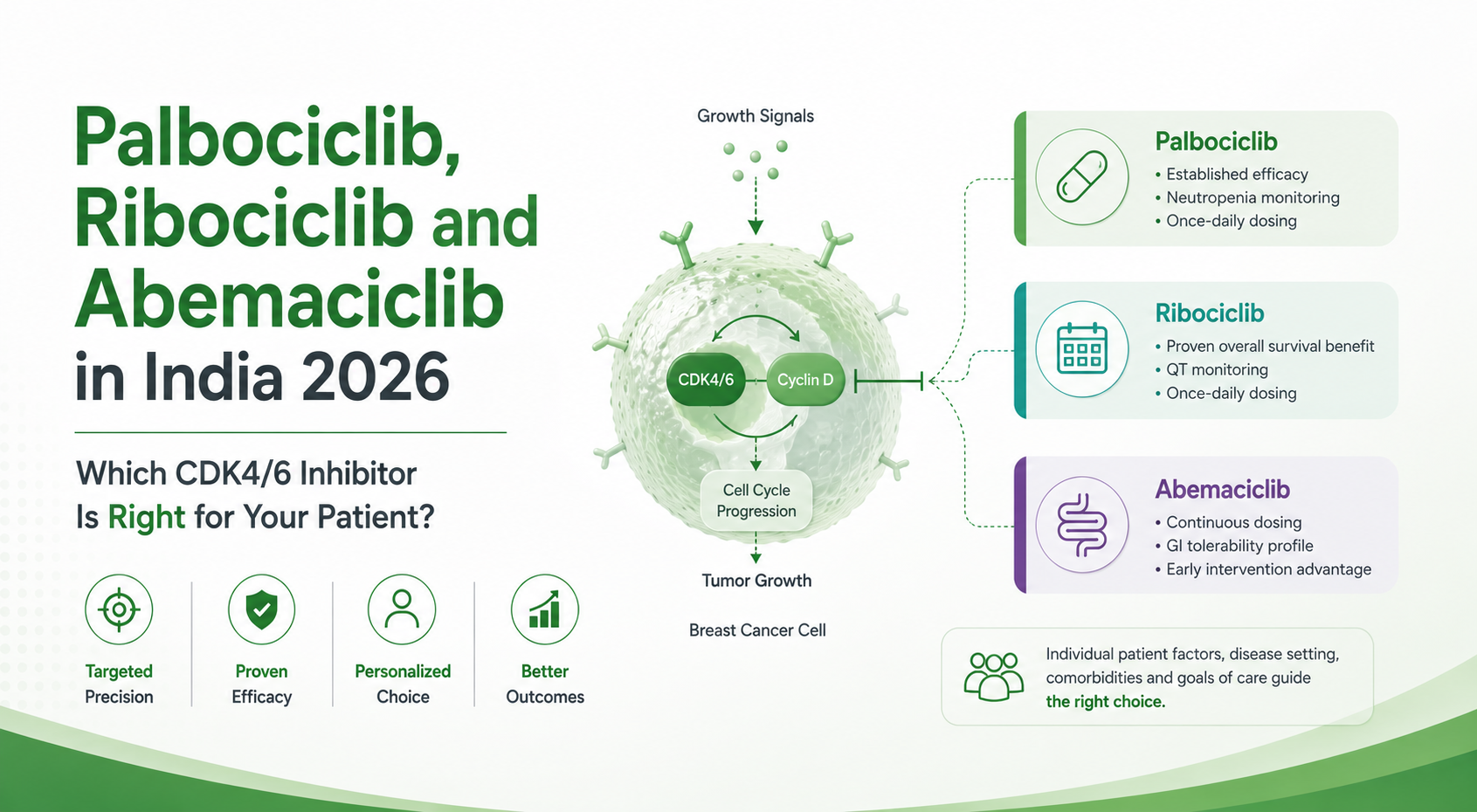
CDK4 and CDK6 are cyclin-dependent kinases — enzymes that drive the transition from G1 to S phase in the cell cycle, the point at which a cell commits to DNA replication and division. In HR+/HER2- breast cancer, estrogen receptor signalling continuously activates CDK4/6 via cyclin D1 upregulation — driving relentless cancer cell proliferation.
Endocrine therapy (aromatase inhibitors, Fulvestrant) reduces the estrogen signal that activates this pathway. CDK4/6 inhibitors block the pathway directly — preventing Rb phosphorylation, arresting the cell cycle at G1, and inducing cancer cell senescence. The combination addresses both the upstream signal (endocrine therapy) and the downstream effector (CDK4/6 inhibitors) simultaneously — which is why the combination consistently outperforms endocrine therapy alone.
A comprehensive review published in Oncology Reports in March 2026 confirmed all three approved CDK4/6 inhibitors demonstrate significant improvements in progression-free survival when combined with endocrine therapy in HR+/HER2- breast cancer. However, as Nature Reviews Clinical Oncology noted in May 2026, resistance mechanisms remain a primary clinical challenge — which makes the choice of initial CDK4/6 inhibitor and the sequencing of subsequent therapy increasingly important.
The Three Agents — Evidence, Differences, and India Availability
Palbociclib — Palbace — 75mg, 100mg, 125mg Capsules
Palbociclib was the first CDK4/6 inhibitor approved — FDA approval in 2015 — and carries the longest clinical follow-up data of any agent in this class. The PALOMA-2 trial demonstrated significant PFS improvement vs Letrozole alone in first-line metastatic HR+/HER2- breast cancer, and PALOMA-3 established efficacy after prior endocrine therapy with Fulvestrant.
In 2026, Palbociclib remains the most widely prescribed CDK4/6 inhibitor in India — partly due to the availability of generic versions at accessible pricing, and partly due to the depth of prescriber familiarity built over a decade of clinical use.
Key characteristics:
- Dose: 125mg once daily, 21 days on / 7 days off
- Partner: Aromatase inhibitor (Arimidex, Letrozole) first-line or Fulvestrant (Faslodex) after prior endocrine therapy
- PFS benefit: Significant vs endocrine therapy alone across all PALOMA trials
- OS benefit: Not significantly demonstrated in Phase 3 — an important distinction vs Ribociclib and Abemaciclib
- Neutropenia: Most common Grade 3-4 adverse event (~66%) — requires CBC monitoring but rarely causes serious infection
- No continuous dosing — the 7-day break distinguishes Palbociclib from Abemaciclib
Ribociclib — Kryxana — 200mg Tablets
Ribociclib has the strongest overall survival data of the three CDK4/6 inhibitors — and this distinction is clinically significant. The MONALEESA-2 trial demonstrated significant OS benefit with Ribociclib + Letrozole in first-line postmenopausal metastatic breast cancer — a 12.4-month improvement in median OS. MONALEESA-7 demonstrated OS benefit in premenopausal patients with ovarian suppression — the first CDK4/6 inhibitor trial to show this specifically in premenopausal women. MONALEESA-3 demonstrated OS benefit with Ribociclib + Fulvestrant.
This consistent OS benefit across three Phase 3 trials in different patient populations makes Ribociclib the CDK4/6 inhibitor with the most robust survival evidence.
Key characteristics:
- Dose: 600mg once daily, 21 days on / 7 days off (3 tablets of 200mg)
- Partner: Aromatase inhibitor or Faslodex (Fulvestrant) — valid in premenopausal patients with ovarian suppression (Zoladex/Goserelin)
- OS benefit: Significant across MONALEESA-2, -3, and -7
- QTc prolongation: Mandatory ECG monitoring at baseline, 2 weeks, and 4 weeks. Avoid in patients with pre-existing QTc prolongation
- Hepatotoxicity: Monitor LFTs — Grade 3-4 ALT/AST elevation in approximately 9%
- Premenopausal indication: Uniquely validated in MONALEESA-7
Abemaciclib — Ramiven — 50mg, 100mg, 150mg, 200mg Tablets
Abemaciclib is the most structurally distinctive of the three CDK4/6 inhibitors. It is the only CDK4/6 inhibitor approved for continuous twice-daily dosing (no off-week), it can be used as monotherapy in certain heavily pretreated patients, and it is the only CDK4/6 inhibitor approved for adjuvant use in high-risk early breast cancer.
MONARCH 2 demonstrated OS benefit with Abemaciclib + Fulvestrant in second-line metastatic HR+/HER2- breast cancer. The monarchE trial established Abemaciclib + endocrine therapy as adjuvant treatment for high-risk HR+/HER2- node-positive early breast cancer — with sustained benefit at 5 years.
Key characteristics:
- Dose: 150mg twice daily continuously (no off-week) — metastatic; 150mg twice daily for 2 years — adjuvant (monarchE)
- Partner: Aromatase inhibitor first-line; Fulvestrant second-line; endocrine therapy adjuvant
- OS benefit: Significant in MONARCH 2 (second-line metastatic with Fulvestrant)
- Diarrhoea: Most common and distinguishing side effect (~85% any grade, ~13% Grade 3) — prophylactic Loperamide at treatment initiation is standard
- Adjuvant indication: The only CDK4/6 inhibitor approved for early breast cancer adjuvant use
- Monotherapy option: Approved in heavily pretreated metastatic HR+/HER2- breast cancer
Head-to-Head Comparison
| Feature | Palbace (Palbociclib) | Kryxana (Ribociclib) | Ramiven (Abemaciclib) |
|---|---|---|---|
| Dosing schedule | 21 on / 7 off | 21 on / 7 off | Continuous twice daily |
| First-line metastatic | ✅ PALOMA-2 | ✅ MONALEESA-2 | ✅ MONARCH 3 |
| Second-line metastatic | ✅ PALOMA-3 | ✅ MONALEESA-3 | ✅ MONARCH 2 |
| OS benefit demonstrated | ❌ Not significant | ✅ MONALEESA-2, -3, -7 | ✅ MONARCH 2 |
| Premenopausal indication | ❌ No | ✅ MONALEESA-7 | Limited data |
| Adjuvant early breast cancer | ❌ No | ❌ No | ✅ monarchE |
| Monotherapy option | ❌ No | ❌ No | ✅ Yes |
| Main side effect | Neutropenia | Neutropenia + QTc | Diarrhoea |
| QTc monitoring needed | ❌ No | ✅ Yes — mandatory | ❌ No |
| Available at A.K. Pharma | Palbace | Kryxana | Ramiven |
Which Patients Benefit Most From Each Agent
Choose Palbociclib (Palbace) when:
- Cost accessibility is the primary consideration
- First-line postmenopausal HR+/HER2- metastatic breast cancer with Letrozole or Anastrozole
- Patients where QTc monitoring infrastructure is limited
- Established prescriber familiarity preferred
Choose Ribociclib (Kryxana) when:
- Overall survival benefit is the priority — MONALEESA data is the most consistent
- Premenopausal patients requiring CDK4/6 inhibitor + ovarian suppression (Zoladex) — MONALEESA-7 validated this specifically
- Both first-line (with AI) and second-line (with Faslodex) settings
Choose Abemaciclib (Ramiven) when:
- High-risk early breast cancer — node-positive HR+/HER2- — adjuvant use per monarchE
- Second-line metastatic with Faslodex — MONARCH 2 OS benefit
- Heavily pretreated metastatic patients where monotherapy is being considered
- Patients where neutropenia avoidance is a priority
CDK4/6 Inhibitors and PIK3CA Mutations — When to Add Alpelisib
For patients who progress on CDK4/6 inhibitor + endocrine therapy and have a PIK3CA mutation confirmed by NGS, Pivikto (Alpelisib) + Faslodex (Fulvestrant) is a validated next-line option — demonstrated in the BYLieve trial which specifically enrolled post-CDK4/6i patients. PIK3CA testing at diagnosis or at progression is therefore increasingly important in Indian oncology practice.
Pre-Treatment Considerations Specific to India
Confirm menopausal status before selecting aromatase inhibitor combinations. Aromatase inhibitors are ineffective in premenopausal women without ovarian suppression. For premenopausal patients, Ribociclib + Zoladex (Goserelin) + AI or Fulvestrant has the strongest evidence from MONALEESA-7.
QTc monitoring for Ribociclib. Baseline ECG and ECG at weeks 2 and 4 required. In centres where ECG access between consultations is limited, Palbociclib or Abemaciclib may be more practical.
Diarrhoea management for Abemaciclib. Prophylactic Loperamide at treatment initiation significantly reduces Grade 3-4 severity. Patient counselling before starting is essential.
PIK3CA testing — plan ahead. India’s oncology infrastructure is expanding rapidly — Metropolis Healthcare’s Centre of Genomics opened in February 2026 specifically to accelerate personalised cancer diagnostics. Tissue NGS or plasma liquid biopsy for PIK3CA status should be incorporated at diagnosis — not only at progression.
Managing CDK4/6 Inhibitor Side Effects
Neutropenia (Palbociclib and Ribociclib): Grade 3-4 in ~60-66%. Febrile neutropenia is uncommon (<2%) — uncomplicated neutropenia without fever does not require dose reduction on first occurrence. CBC every 2 weeks for first 2 cycles, then monthly.
Diarrhoea (Abemaciclib): Start Loperamide 4mg at first loose stool. Dietary modification in first month. Grade 3+ — hold Abemaciclib; restart at reduced dose when resolved to Grade 1.
QTc prolongation (Ribociclib): Baseline ECG. Correct electrolytes before starting. Avoid concomitant QTc-prolonging medicines including ondansetron, domperidone, antifungals. Withhold for QTc >480ms.
Hepatotoxicity (all three): LFTs at baseline, every 2 weeks for first 2 cycles, then monthly. Withhold for Grade 3; permanently discontinue for Grade 4.
A.K. Pharma — Pharmaceutical Distributor in Delhi for the Complete Breast Cancer Portfolio
A.K. Pharma is a licensed medicine distributor and pharmaceutical distributor in Delhi supplying the complete HR+/HER2- breast cancer targeted therapy portfolio — all three CDK4/6 inhibitors, their endocrine therapy partners, and the post-CDK4/6i options — to hospitals, oncology centres, and pharmacies across India.
CDK4/6 Inhibitors:
- Palbace (Palbociclib) — 75mg, 100mg, 125mg capsules
- Kryxana (Ribociclib) — 200mg tablets
- Ramiven (Abemaciclib) — 50mg, 100mg, 150mg, 200mg tablets
Endocrine Therapy Partners:
- Arimidex (Anastrozole) — aromatase inhibitor
- Aromasin (Exemestane) — aromatase inhibitor
- Faslodex (Fulvestrant) — SERD
- Zoladex (Goserelin) — GnRH agonist for premenopausal OFS
Post-CDK4/6i Options:
- Pivikto (Alpelisib) — PI3Kα inhibitor for PIK3CA-mutated HR+/HER2- metastatic breast cancer
Browse our complete cancer medicines or contact us directly.
📍 E-2/257A, 2nd Floor, Shastri Nagar, New Delhi 110052
📞 011 4172 6999
📱 WhatsApp: +91 9810034827
Frequently Asked Questions
Q. What is the difference between Palbociclib, Ribociclib, and Abemaciclib?
All three are CDK4/6 inhibitors for HR+/HER2- breast cancer but differ in key ways. Ribociclib has the strongest and most consistent OS data. Abemaciclib is the only one approved for adjuvant early breast cancer and for monotherapy. Palbociclib is the most widely prescribed, most accessible generically, and requires no QTc monitoring.
Q. Which CDK4/6 inhibitor has proven overall survival benefit?
Q. Can CDK4/6 inhibitors be used in premenopausal women?
Yes — Ribociclib (Kryxana) specifically has Phase 3 OS data in premenopausal women from MONALEESA-7, used with ovarian function suppression (Zoladex/Goserelin) and aromatase inhibitor or Fulvestrant.
Q. Is Abemaciclib used differently from Palbociclib and Ribociclib?
Yes — Abemaciclib (Ramiven) is taken continuously twice daily (no off week), is approved for adjuvant use in high-risk early breast cancer (monarchE), can be used as monotherapy, and causes primarily diarrhoea rather than neutropenia.
Q. What happens after CDK4/6 inhibitor progression?
For PIK3CA-mutated patients, Pivikto (Alpelisib) + Faslodex (Fulvestrant) is a validated option. PIK3CA testing at diagnosis or progression is essential to prepare for this decision.
Q. Are all three CDK4/6 inhibitors available in India?
Yes — A.K. Pharma is a licensed pharmaceutical distributor in Delhi supplying Palbace, Kryxana, and Ramiven (Abemaciclib) to hospitals, oncology centres, and pharmacies across India. Contact us at 011 4172 6999 or WhatsApp +91 9810034827.